Heart chambers:
The heart consists of two pumps which are separated by a partition. The right pump receives deoxygenated blood from the human body and sends this blood into the lungs, while the left pump receives oxygenated blood from the lungs and pumps it into the systemic circulation.
Right atrium (Fig.4):
This chamber forms the most anterior surface of the heart. The blood returns from the systemic circulation into this chamber by three main vessels:
- The superior vena cava, which enters the upper portion of the right atrium and delivers the blood from the upper body and head into the heart.
- The inferior vena cava which enters the lower portion of the right atrium and delivers the blood from the lower body and legs.
- The coronary sinus which enters the lower portion of the right atrium and delivers the blood from the heart wall itself.
The blood then passes through the right atrioventricular orifice via the tricuspid valve, from the right atrium to the right ventricle. The anterior right atrium has two continuous spaces separated by an external vertical groove (the sulcus terminalis cordis) that extends from the right side of the superior vena cava to the right side of the inferior vena cava. In addition, a smooth muscular ridge on the atrium's roof, known as the crista terminalis, indicates this division internally. Posterior to this lies the sinus of the vena cavae, which is derived from the right horn of the sinus venosus in fetal life. The anterior space of the crista includes the right auricle which is covered by the musculi pectinati (pectinate muscles). Small folds in the wall of the right atrium are derived from the valve of the embryonic sinus venosus (the valves of the coronary sinus and inferior vena cava). In addition, the interatrial septum separating the right and left atria has a small depression known as the fossa ovalis (oval fossa), just above the orifice of the inferior vena cava. Finally, the smallest cardiac veins drain the myocardium directly into the right atrium via small openings known as foramina of the venae cordis minimae.
Right atrium (Fig.4):
This chamber forms the most anterior surface of the heart. The blood returns from the systemic circulation into this chamber by three main vessels:
- The superior vena cava, which enters the upper portion of the right atrium and delivers the blood from the upper body and head into the heart.
- The inferior vena cava which enters the lower portion of the right atrium and delivers the blood from the lower body and legs.
- The coronary sinus which enters the lower portion of the right atrium and delivers the blood from the heart wall itself.
The blood then passes through the right atrioventricular orifice via the tricuspid valve, from the right atrium to the right ventricle. The anterior right atrium has two continuous spaces separated by an external vertical groove (the sulcus terminalis cordis) that extends from the right side of the superior vena cava to the right side of the inferior vena cava. In addition, a smooth muscular ridge on the atrium's roof, known as the crista terminalis, indicates this division internally. Posterior to this lies the sinus of the vena cavae, which is derived from the right horn of the sinus venosus in fetal life. The anterior space of the crista includes the right auricle which is covered by the musculi pectinati (pectinate muscles). Small folds in the wall of the right atrium are derived from the valve of the embryonic sinus venosus (the valves of the coronary sinus and inferior vena cava). In addition, the interatrial septum separating the right and left atria has a small depression known as the fossa ovalis (oval fossa), just above the orifice of the inferior vena cava. Finally, the smallest cardiac veins drain the myocardium directly into the right atrium via small openings known as foramina of the venae cordis minimae.
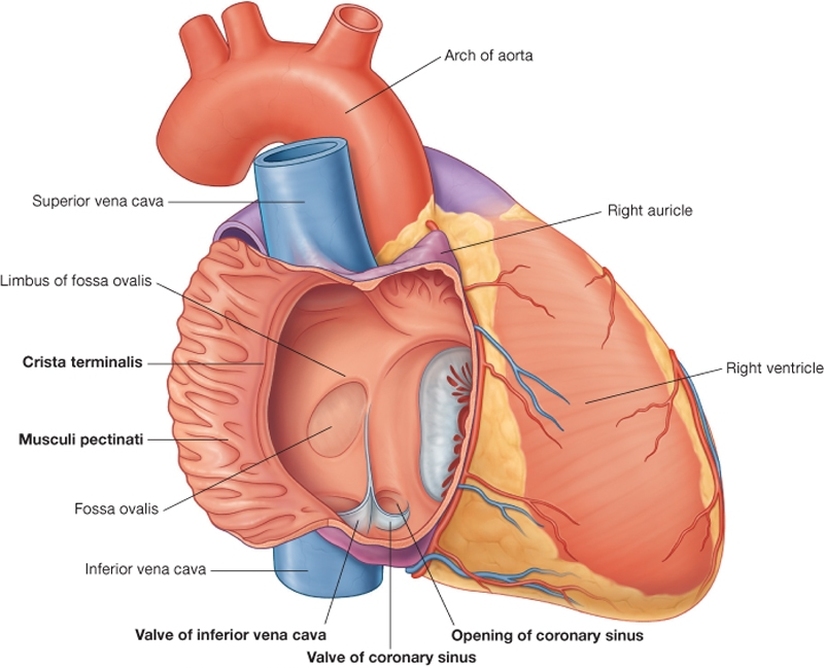
Figure.4: The right atrium (Drake et al, 2009).
The right ventricle (Fig.5):
The right ventricle wall is thicker than that of the right atrium. This chamber communicates with the right atrium and pulmonary trunk by the atrioventricular orifice and the pulmonary orifice respectively. The outflow tract to the pulmonary trunk is known as the conus arteriosus (infundibulum). The right ventricular wall contains muscular bundles forming internal projecting ridges known as the trabeculae carneae; these are composed of three types. The first forms the papillary muscles which attach to the ventricle wall at their bases and to the tricuspid valve by the chordae tendineae at their apices. The second are attached to the wall of the right ventricle but are free in the middle, e.g. the moderator band which crosses the ventricular cavity from the septal to the anterior wall. Finally, the third has prominent ridges.
The right ventricle wall is thicker than that of the right atrium. This chamber communicates with the right atrium and pulmonary trunk by the atrioventricular orifice and the pulmonary orifice respectively. The outflow tract to the pulmonary trunk is known as the conus arteriosus (infundibulum). The right ventricular wall contains muscular bundles forming internal projecting ridges known as the trabeculae carneae; these are composed of three types. The first forms the papillary muscles which attach to the ventricle wall at their bases and to the tricuspid valve by the chordae tendineae at their apices. The second are attached to the wall of the right ventricle but are free in the middle, e.g. the moderator band which crosses the ventricular cavity from the septal to the anterior wall. Finally, the third has prominent ridges.
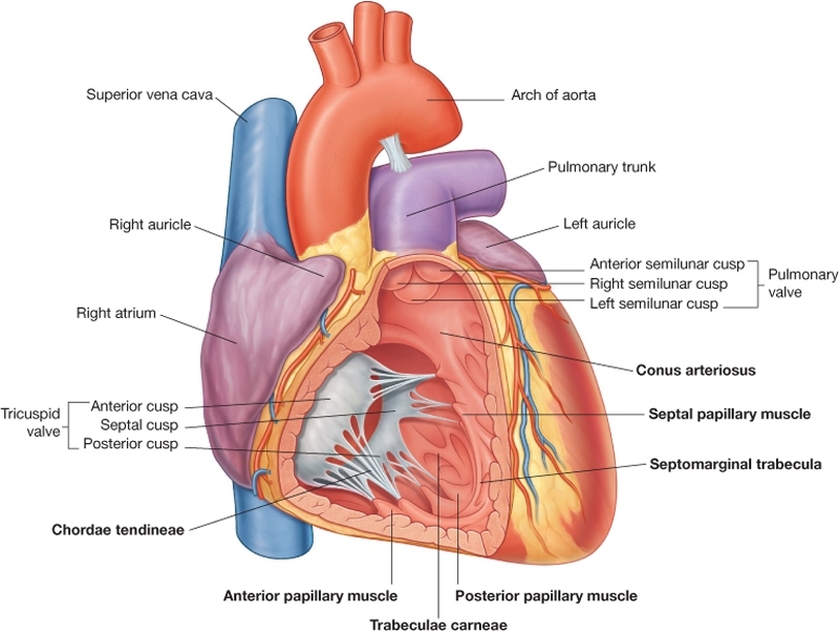
Figure.5: The right ventricle (Drake et al, 2009).
The left atrium (Fig.6):
The basal or posterior surface of the heart is formed by the left atrium, being derived from two structures developmentally:
- A posterior half known as the inflow portion, because it receives blood from the four pulmonary veins: this part has smooth walls.
- An anterior half which is continuous with the left auricle and contains musculi pectinati.
The interatrial septum forms part of the anterior wall and has the depression that forms the valve of the foramen ovale: directly opposite the floor of the fossa ovalis in the right atrium.
The basal or posterior surface of the heart is formed by the left atrium, being derived from two structures developmentally:
- A posterior half known as the inflow portion, because it receives blood from the four pulmonary veins: this part has smooth walls.
- An anterior half which is continuous with the left auricle and contains musculi pectinati.
The interatrial septum forms part of the anterior wall and has the depression that forms the valve of the foramen ovale: directly opposite the floor of the fossa ovalis in the right atrium.
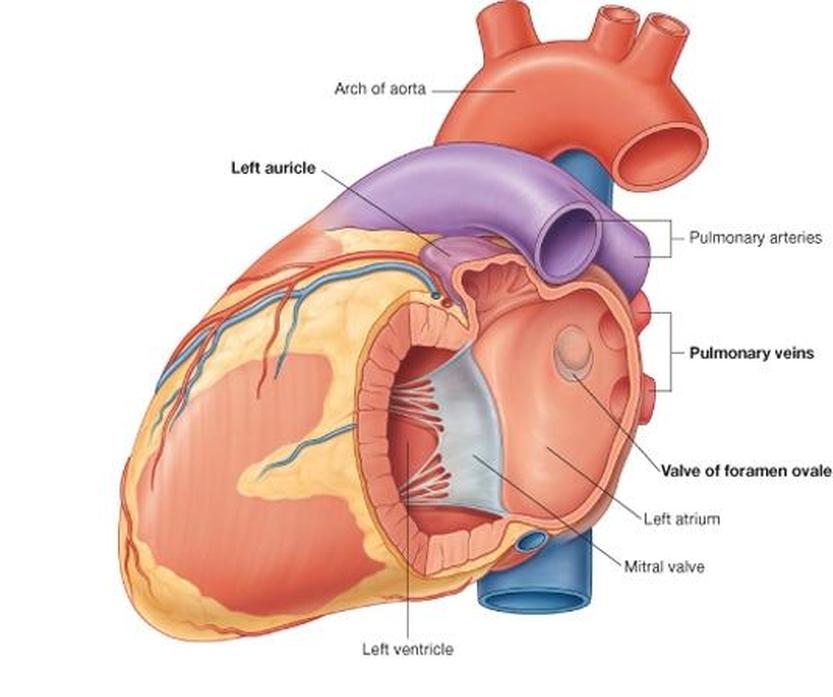
Figure.6: The left atrium (Drake et al, 2009).
The left ventricle (Fig.7):
The left ventricle is longer than the right ventricle with the thickest layer of myocardium. It lies anterior to the left atrium, and forms the apex of the heart. The blood enters the left ventricle by passing through the left atrioventricular orifice, guarded by the mitral valve. Posterior to the infundibulum of the right ventricle, the left ventricle outflow tract is known as the aortic vestibule and has smooth walls: it is derived from the bulbus cordis.
In addition, the trabeculae carneae of the left ventricle are finer and more delicate than those in the right ventricle. Here too, papillary muscles connect to the cusped leaflets by chordae tendineae as in the right ventricle. There are two papillary muscles groups here, the anterior and posterior papillary muscles: they are generally larger than those found in the right ventricle.
Depending on the anatomical location of the heart, the left ventricle is usually posterior to the right ventricle; they are separated by the interventricular septum which forms the anterior wall and some of the wall on the right side of the left ventricle. The septum is divided into two parts:
- A thick muscular part, which forms the main part of the septum
- A thinner membranous part.
The left ventricle is longer than the right ventricle with the thickest layer of myocardium. It lies anterior to the left atrium, and forms the apex of the heart. The blood enters the left ventricle by passing through the left atrioventricular orifice, guarded by the mitral valve. Posterior to the infundibulum of the right ventricle, the left ventricle outflow tract is known as the aortic vestibule and has smooth walls: it is derived from the bulbus cordis.
In addition, the trabeculae carneae of the left ventricle are finer and more delicate than those in the right ventricle. Here too, papillary muscles connect to the cusped leaflets by chordae tendineae as in the right ventricle. There are two papillary muscles groups here, the anterior and posterior papillary muscles: they are generally larger than those found in the right ventricle.
Depending on the anatomical location of the heart, the left ventricle is usually posterior to the right ventricle; they are separated by the interventricular septum which forms the anterior wall and some of the wall on the right side of the left ventricle. The septum is divided into two parts:
- A thick muscular part, which forms the main part of the septum
- A thinner membranous part.
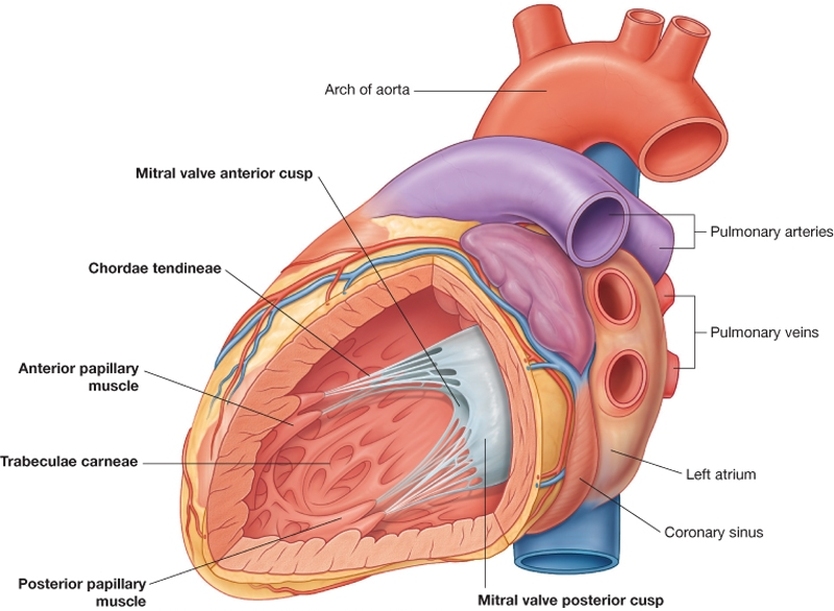
Figure.7: The left ventricle (Drake et al, 2009).
Heart valves (Fig, 5, 6 & 7):
Tricuspid and mitral valves:
The tricuspid valve consists of three cusps anterior, septal and inferior (posterior). These cusps are formed by a fold of the endocardium and some connective tissue. The bases of the cusps attach to the fibrous ring of the heart skeleton and their free edges attach to the chordae tendineae connecting them to the papillary muscles.
The mitral valve consists of two cusps anterior and posterior: its structure is similar to the tricuspid valve. The anterior cusp is larger and intervenes between the atrioventricular and the aortic orifices. The chordae tendineae attach the cusps to papillary muscles as in the tricuspid valve.
During ventricular contraction, the papillary muscles contract preventing the cusps from being forced into the atrium with rising intraventricular pressure.
The pulmonary valve and aortic valves:
The pulmonary valve consists of three semilunar cusps formed by folds of the endocardium and some connective tissue. The lower margins of the cusps and their sides are attached to the arterial wall. Additionally, the open mouths of these cusps face upwards into the pulmonary trunk forming three sinuses in the root of the pulmonary trunk. There are no chordae tendineae or papillary muscles attached to these valves. The semilunar pulmonary valves are arranged as one posterior (left cusp) and two anterior (anterior and right cusps).
The aortic valve has a similar arrangement to the pulmonary valve, but the valves are arranged as one anterior (right) and two posterior (left and posterior). The aortic sinus is similarly formed from bulging of the aortic wall behind each cusp. The right coronary artery originates from the anterior aortic sinus and the left coronary artery from the left posterior sinus.
During ventricular systole the outrushing blood presses the valves against the wall of the pulmonary trunk and the aorta. However, during diastole the blood flows back to the heart entering the sinuses and filling the pockets formed by valves. As a result, the valves fall into the centre of the lumen and close the pulmonary and aortic orifices.
The tricuspid valve consists of three cusps anterior, septal and inferior (posterior). These cusps are formed by a fold of the endocardium and some connective tissue. The bases of the cusps attach to the fibrous ring of the heart skeleton and their free edges attach to the chordae tendineae connecting them to the papillary muscles.
The mitral valve consists of two cusps anterior and posterior: its structure is similar to the tricuspid valve. The anterior cusp is larger and intervenes between the atrioventricular and the aortic orifices. The chordae tendineae attach the cusps to papillary muscles as in the tricuspid valve.
During ventricular contraction, the papillary muscles contract preventing the cusps from being forced into the atrium with rising intraventricular pressure.
The pulmonary valve and aortic valves:
The pulmonary valve consists of three semilunar cusps formed by folds of the endocardium and some connective tissue. The lower margins of the cusps and their sides are attached to the arterial wall. Additionally, the open mouths of these cusps face upwards into the pulmonary trunk forming three sinuses in the root of the pulmonary trunk. There are no chordae tendineae or papillary muscles attached to these valves. The semilunar pulmonary valves are arranged as one posterior (left cusp) and two anterior (anterior and right cusps).
The aortic valve has a similar arrangement to the pulmonary valve, but the valves are arranged as one anterior (right) and two posterior (left and posterior). The aortic sinus is similarly formed from bulging of the aortic wall behind each cusp. The right coronary artery originates from the anterior aortic sinus and the left coronary artery from the left posterior sinus.
During ventricular systole the outrushing blood presses the valves against the wall of the pulmonary trunk and the aorta. However, during diastole the blood flows back to the heart entering the sinuses and filling the pockets formed by valves. As a result, the valves fall into the centre of the lumen and close the pulmonary and aortic orifices.
Copyright © 2011 by Reem Bu Saeed.
Last updated: 30-07-2011.
Last updated: 30-07-2011.
